SAEDNEWS: Follicles contain cells that produce estrogen for egg growth and maturation. Eggs form during the first week of fetal life, and from the first period onward, higher-quality eggs are selected first, with later cycles yielding lower-quality eggs.
According to SaedNews Family Service, citing NiniSite, many women mistakenly think that a follicle is the same as an egg—but it isn’t. In reality, the female gamete, known as the egg, and the male gamete, sperm, are the cells present in a fertilized embryo after conception.
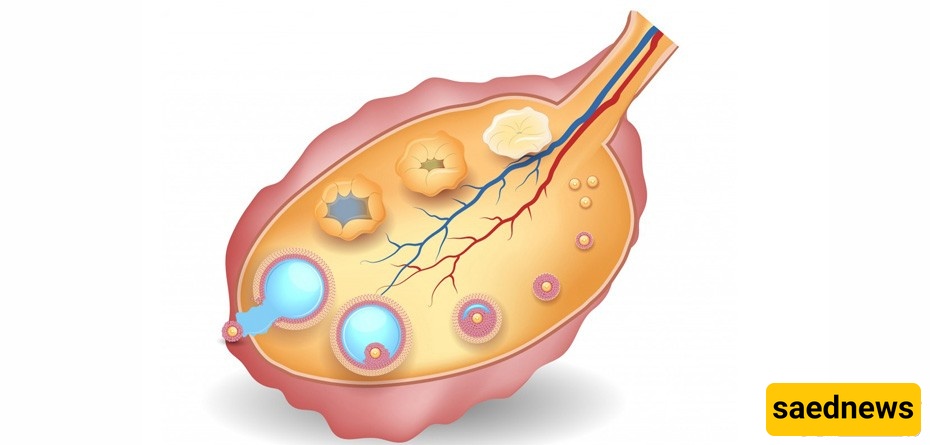
A follicle is a small, round cluster located in the ovary, surrounded by ovarian tissue cells. The egg itself is a cell that, under normal conditions, matures in the microscopic inner wall of the follicle during natural or hormonally stimulated cycles.
Follicles also contain other cells that produce the estrogen necessary for the normal growth and maturation of the egg. Eggs first appear during the initial week of a female fetus’s life. From a girl’s first menstrual period onward, eggs are selected based on quality: higher-quality eggs are chosen first, while eggs from successive cycles gradually have lower quality.
This explains why pregnancy is often more challenging for older women, and why miscarriage rates are higher in this group.
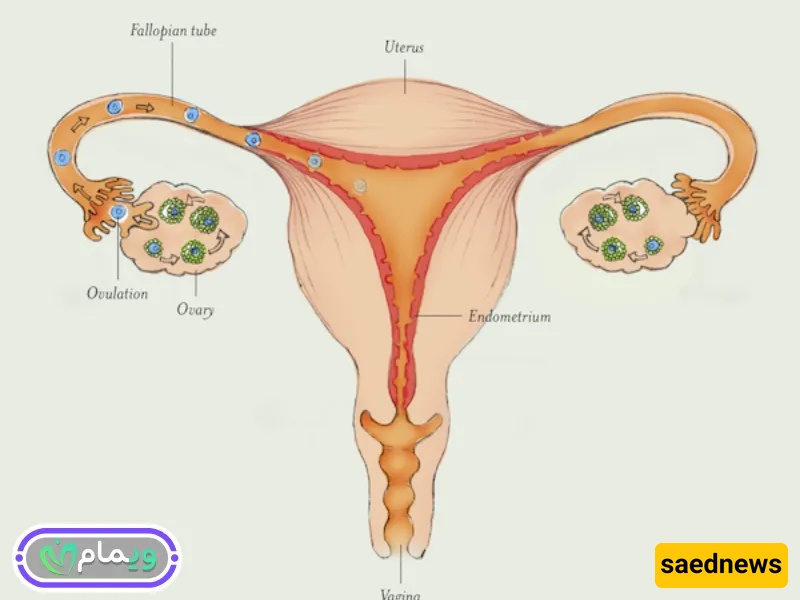
To assess a woman’s fertility, ovarian reserve must be measured. Hormones such as AMH, FSH, LH, and estrogen are analyzed, alongside vaginal ultrasounds. Currently, counting ovarian follicles is the most reliable way to estimate ovarian reserve. This count measures the number of visible follicles in each ovary on the first days of the cycle (days 2–5), using vaginal ultrasound. These are called antral follicles, and ultrasound can track their growth and ovulation status in both natural and induced cycles in infertility treatments.
Follicle Number and Size
6–10 antral follicles indicate a normal ovarian reserve.
Fewer than 6 suggest low reserve, while more than 12 indicate a high reserve.
Follicle size ranges from 2 to 10 mm during the cycle.
Women with low ovarian reserve are less likely to respond to fertility treatments, whereas women with high reserve may respond excessively. In both cases, treatment is often scheduled when antral follicle counts are within a normal range.
In a natural cycle, one antral follicle is selected as the “dominant follicle” due to its size and rapid growth. This follicle, called a Graafian follicle, eventually matures for ovulation. Other follicles undergo atresia, a programmed biological process where they shrink or die.
Before ovulation, the dominant follicle usually measures 22–24 mm, although sizes between 18 and 36 mm have been recorded. Follicle size is a reliable indicator for predicting ovulation.
In a hormonally stimulated cycle, most or all antral follicles grow, though at different rates. When several follicles reach 18 mm, HCG is administered to trigger ovulation. This approach is used in infertility treatments to select the most mature eggs for fertilization.
Follicle growth doesn’t always guarantee a mature egg. Just as not all sperm are capable of fertilization, not all follicles contain mature eggs or eggs of equal quality.
A rare condition, called Empty Follicle Syndrome, affects a small percentage of women undergoing fertility treatment. Despite adequate follicle growth and estradiol levels, no eggs are retrieved during IVF. The exact cause is unknown; potential factors include HCG management, abnormal treatment response, or incomplete follicular maturation.
This syndrome is more common in women with primary infertility—those who have never been pregnant despite a normal follicle count. Though rare (occurring in only 7% of cases), its likelihood increases with age.





























